KAISER
PERMANENTE
The Permanente Medical Group (TPMG) Clinical
Practice Guidelines have been
developed to
assist clinicians by providing an analytical
framework for the evaluation and treatment
of selected
common problems encountered in patients. These
guidelines are not intended to establish
a protocol for all patients with a particular condition. While
the guidelines provide one approach to evaluating
a problem,
clinical conditions may vary significantly from individual to individual.
Therefore, the clinician must
exercise
independent judgment and make decisions based upon the
situation presented. While great care has
been taken
to assure the accuracy of the information presented,
the reader is advised that TPMG cannot be
responsible
for continued currency of the information, for any errors or omissions in
this guideline, or for any
consequences
arising from its use.
PEDIATRIC ASTHMA GUIDELINES TEAM,
1998 REVISION
CLINICAL
LEADERS
Richard
Pastcan, MD: Pediatrics, Napa, Co-Chair
Laura
Prager, MD, Pediatrics. Redwood City, Co-Chair
CPG
TEAM
Thomas
Duprey, RPh, MPA: Pharmacy Operations
Harold
I. Farber, MD: Pediatrics, Vallejo
Al
Haas, MD: Allergy. Santa Rosa
Albin
Leong. MD: Pediatrics, Sacramento
Tracy
Lieu. MD, MPH: Division of Research
Guillermo
Mendoza. MD: Allergy, Vacaville
Diana
Powell, B.A. RCP, RRT: Medicine, Santa Teresa
Greg
Shay, MD: Pediatrics, Oakland
Jennifer
Torresen, MPH: Regional Health Education
CaskeyWeston.
RN; Pediatrics, Oakland
REVIEWERS
Gordon
Garcia. MD: Allergy, South Sacramento
Gabriel
Pino, MD: Pediatrics, Fresno
David
Nunez. MD: Pediatrics, San Francisco
Patricia
Sullivan, MD: Pediatrics, Roseville
DATA
ANALYSIS
Don
Fordham, MPH, TPMG Department of Quality and
Utilization
Patricia
Kipnis, PhD. TPMG Department of Quality
and Utilization
Timothy
Ko, DrPH, TPMG Department of Quality and
Utilization
PROJECT
MANAGEMENT
Laura
Finkler, MPH: TPMG Department of Quality and
Utilization
Patti
Hallam, MPH: Division of Research
Kathleen
Martin: TPMG Department of Quality and Utilization
Laura
Skabowski, MS: TPMG Department of Quality and
Utilization
EDITING
Linda
Bine. TPMG Communications
DESIGN
& PRODUCTION
Gail
Holan. Curvey
Produced
by:
TPMG
Department of Quality and Utilization
Kaiser
Pennanente Northern California
1800
Harrison Street, Ste. 410, Oakland, CA 94612
510-987-2950
or tie-line 8-427-2950
To
obtain more information about KPNC Clinical Practice
Guidelines, printed copies,
or permission
to
reproduce
any portion, please contact
the TPMG
Dept.
of Quality & Utilization, or send an e-mail message
to
clinical.guidelines@ncal.kaiperm.org.
Within
the KPNC Lotus Notes network mail to clinical
guidelines or kpnc-cpg. The
Clinical Practice Guidelines for
the Management
of
Asthma in Children are accompanied by a Tool Kit which
you can request. It contains
dosage charts, treatment
algorithms, and practical
tips to asist
clinicians
in their practice. KPNC
Clinical Practice Guidelines can
be viewed online
on the Kaiser Permanente Northern California
intranet
website at hffp://clinical-library.ca.kp.org. This
website is accessible only from
the Kaiser Permanente
computer network. Contents
INTRODUCTION
NEW INFORMATION
& KEY
DIFFERENCES
FROM
THE
1995
GUIDELINE KEY
PRINCIPLES OF PEDIATRIC ASTHMA
MANAGEMENT GOALS
OF ASTHM\
MANAGEMENT
DIAGNOSIS
OF ASTHMA ASSESSMENT
&
CLASSIFICATION OF DISEASE SEVERITY
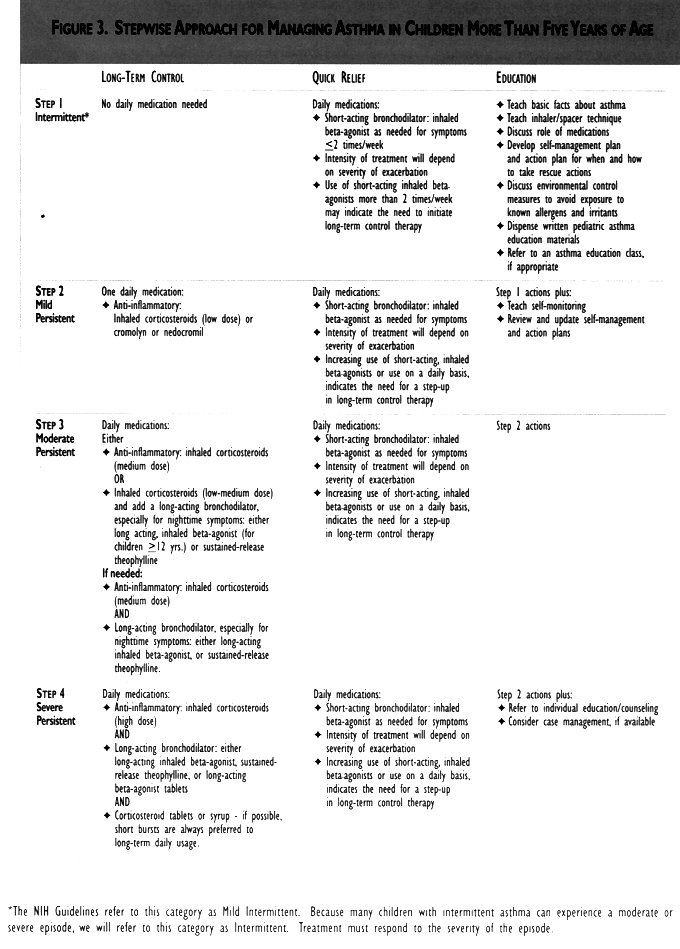
DRUG THERAPY
LONG-TERM AND QUICK RELIEF THERAPY STEPWISE
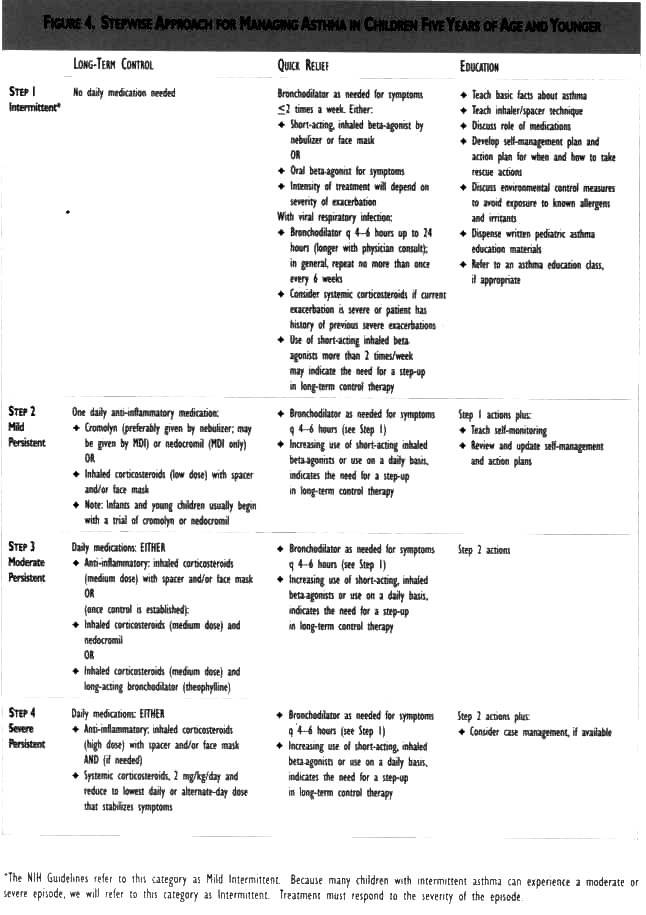
APPROACH TO DRUG THERAPY SPECIAL
CONSIDERATIONS FOR INFANTS AND YOUNG
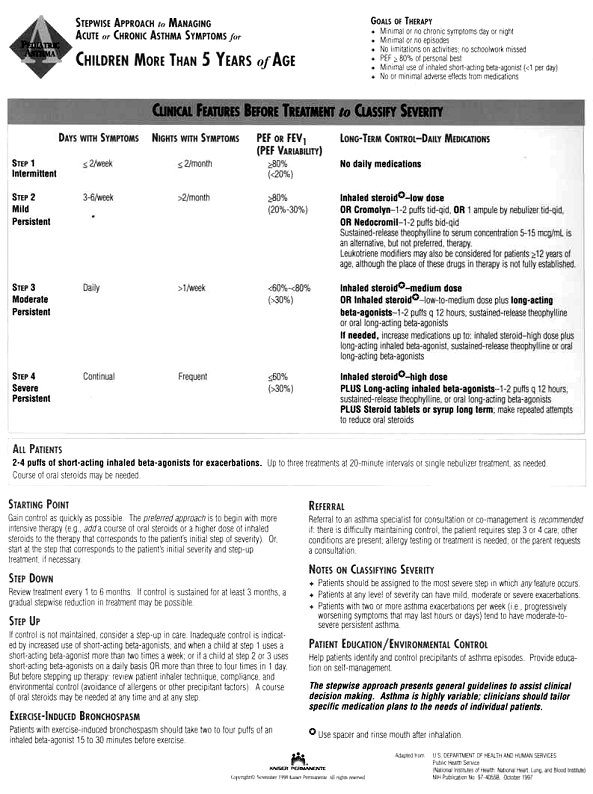
CHILDREN Figure 3: STEPWISE APPROACH FOR MANAGING ASTHMA IN CHILDREN MORE THAN FIVE YEARS OF AGE
Figure
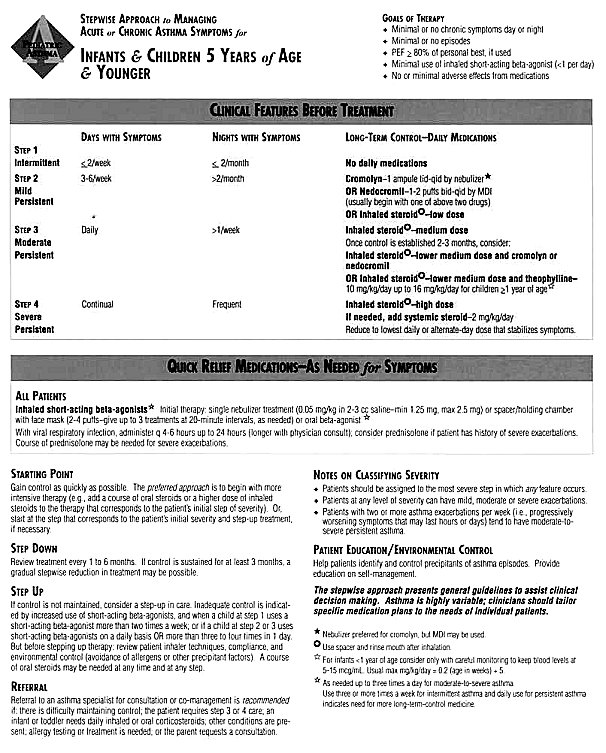
4: STEPWISE APPROACH FOR MANAGING
ASTHMA IN
CHILDREN FIVE
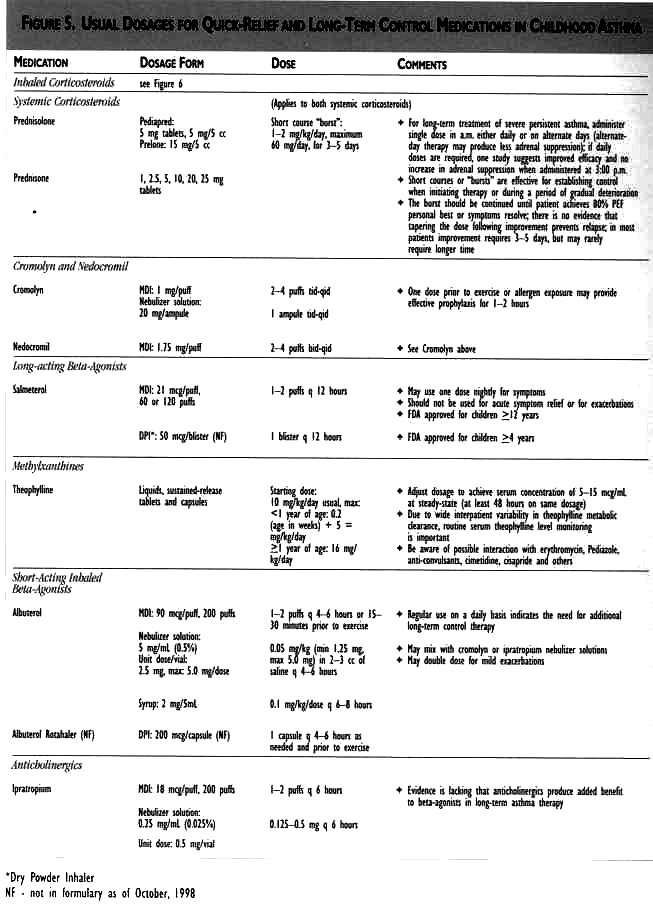
YEARS OF AGE AND YOUNGER Figure
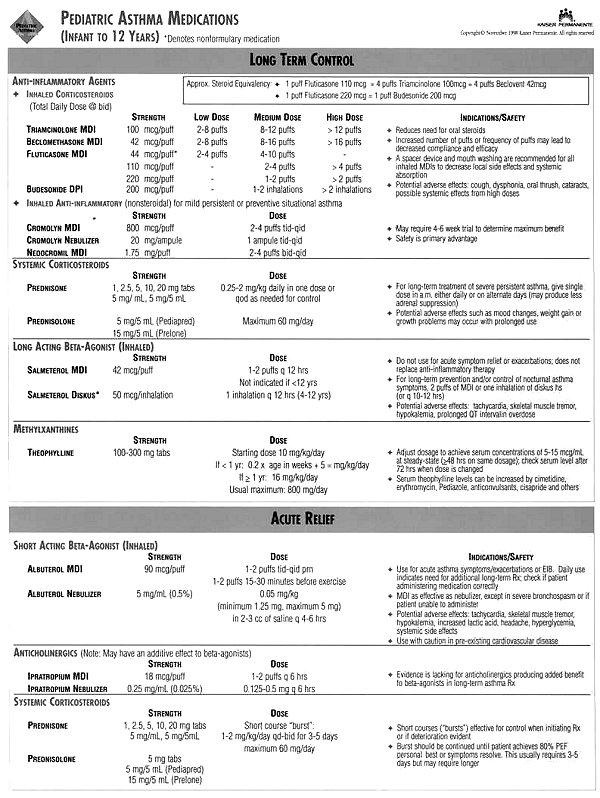
5: Usual Dosages for Quick-Relief and
Long-Term Control
Medications in Childhood
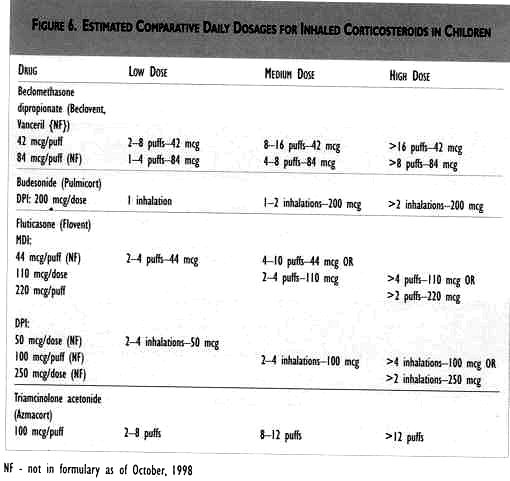
Asthma Figure 6: Estimated Daily Dosages
for Inhaled
Corticosteroids in Children CONTROL OF FACTORS
CONTRIBUTING TO ASTHMA SEVERITY
IMMUNOTHERAPY
IMMUNIZATIONS
WRITTEN PLANS FOR ASTHMA
SELF-MANAGEMENT
EDUCATION FOR A PARTNERSHIP
IN ASTHMA CARE
PERIODIC ASSESSMENT &
MONITORING
INDICATIONS
FOR REASSESSMENT
OR REFERRAL
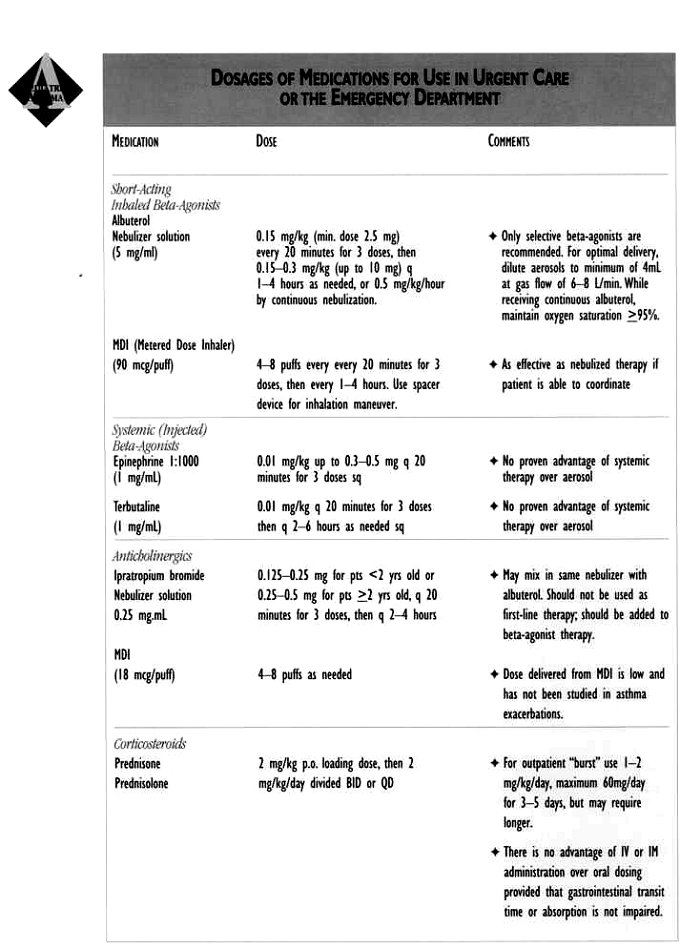
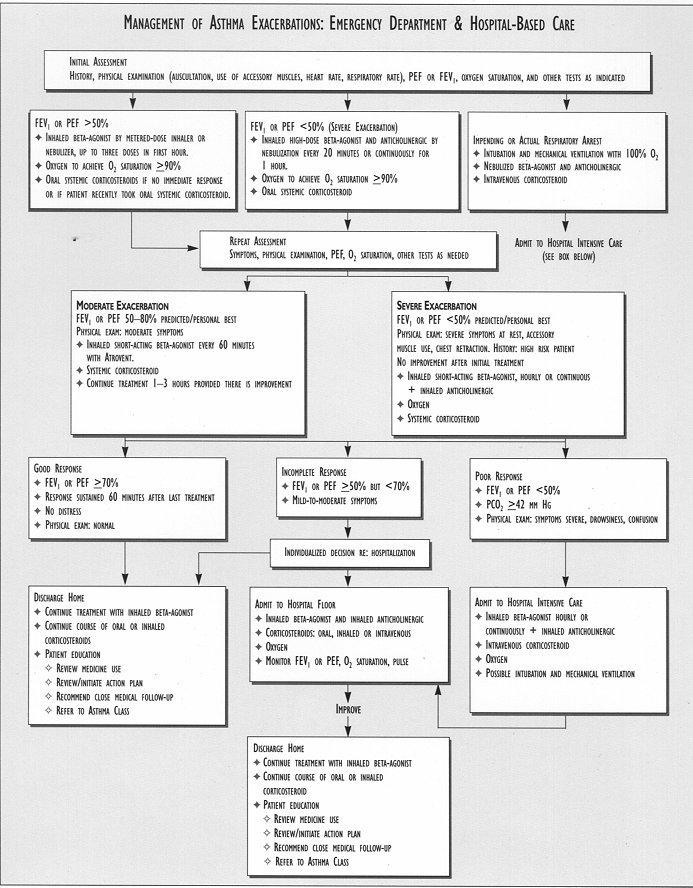
TREATMENT
OF ACUTE
EXACERBATIONS
BIBLIOGRAPHY
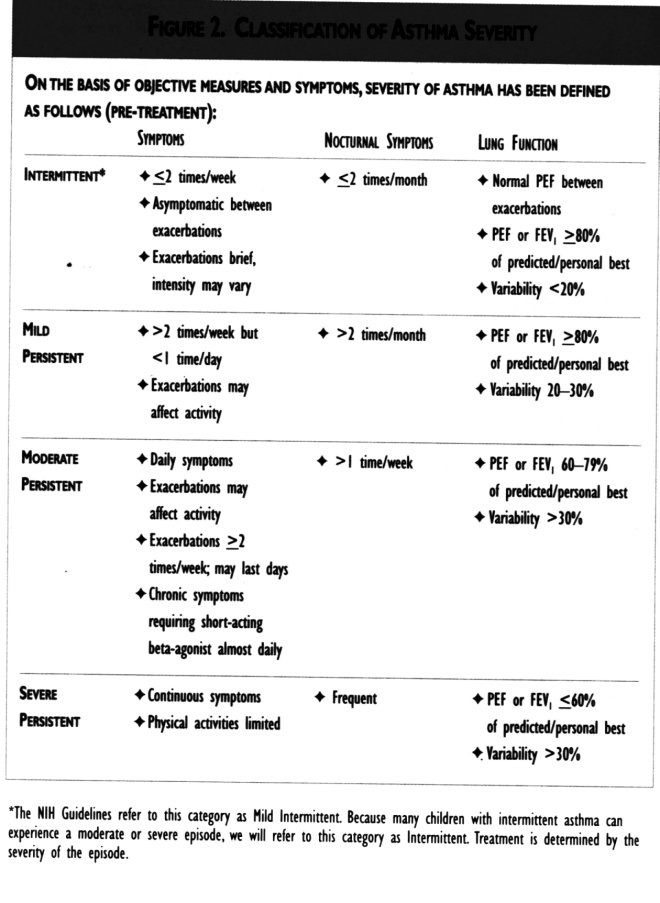
Asthma severity is now classified into four
categories:
intermittent*, mild persistent*,
moderate persistent, and
severe persistent. KPNC
Clinical Practice Guidelines can he viewed
on-line
on the Kaiser
Permanente
Northern California
intranet webbsite at http://clincal-library.ca.kp.org.
These
guidelines have been developed by the
Regional Pediatric
Asthma Guideline Team, an
interdisciplinary
group
charged with developing and overseeing
the implementation of
recommendations
for the
ambulatory treatment of children
with asthma. In developing these
recommendations, team members
reviewed clinical literature,
existing guidelines, and
internal
practices and
outcomes. The approach endorsed
here is based on the 1997 National
Asthma Education and
Prevention Program's Guidelines
for the Diagnosis and Management of
Asthma (referred to as the NIH
[National Institutes of
Health] Guidelines in this document) and is
consistent with other recent
national and international
guidelines
These
Clinical Practice Guidelines will be
reviewed and
revised as necessary on a regular basis,
approximately every two years.
Additional information
on each topic can be
found
in the NIH Guidelines,
which are available in your
facilities Health Services Library. The NIH
Guidelines can also be located
on the internet at
http://www.nhlbi.nih.gov/nhlbi/lung/asthma/prof/asthgdln.htm.
You will need to activate the
Adobe Acrobat Reader which
is available at no cost
via
http://www.adobe.com/prodindex/acrobat/readstep.html.
NEW
INFORMATION and KEY DIFFERENCES from the 1995
GUIDELINE
There
is strong evidence that
asthma is a chronic inflammatory
disorder of the airways,
resulting
from complex
interactions among inflammatory
cells, mediators, and other cells
and tissues resident in the
airways. Asthma medications are now classified as either
long-term
control (preventer) or quick-relief
(reliever) medications. There
is a stronger emphasis
on the use of anti-inflammatory
medications, particularly
inhaled corticosteroids, for
control of persistent asthma. There
is increased emphasis on the fundamental
importance
of an accurate
asthma
diagnosis in order to
manage symptoms effectively.
Asthma severity is now
classified
into four
categories: intermittent*, mild
persistent, moderate persistent, and severe
persistent. Education
should be integrated
into every
step of asthma care. The
patient's active role in managing his/her
asthma is
emphasized, as is the partnership
between the patient and
members of the health care team. Ongoing
monitoring, including self-monitoring and
self-management
tools, is stressed. School
and/or
child care action plans
are recommended. There
is more emphasis on meeting patients' and
families'
expectations of their asthma care. There
are more specific recommendations for
allergy testing
to identify specific triggers, for
when to consider
immunotherapy, and for referral to a
specialist. The NIH Guidelines refer to this category as Mild
Intermittent.
Because many children with
intermittent
asthma can
experience a moderate or severe
episode, we will refer to this category as
Intermittent. Treatment is
determined by severity of
the episode.
KEY PRINCIPLES of PEDIATRIC ASTHMA MANAGEMENT
Since asthma is a
chronic disease, it is especially
important that a patient have a
primary physician, or other
health professional, to manage
his or her health care. Prompt
reassessment of asthma management is needed
after
any asthma-related
hospitalization,
or emergency
department, after-hours,
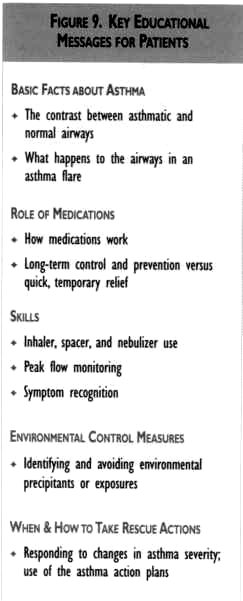
or urgent care visit. Key
educational messages should be integrated into
every
step of asthma care. The principal
clinician should introduce the
concepts, and other members
of the patient care team should
reinforce and expand on them
at every opportunity (see
Figure 9). Peak flow rates should be routinely
documented in
the clinic during follow-up visits when the
patient is asymptomatic. These
values eventually will
provide a baseline against which
peak flow changes can be
compared. Written plans should be developed
together with
the family to help the patient determine: when
and how to step-up
anti-inflammatory medications; when
to start bursts of oral
steroids:
and when to seek
help. In addition to a daily
self-management and action plan, a
plan should be prepared for
the patient's school or child
care center, emphasizing reliable and
prompt access to medications.
Appropriate
anti-inflammatory management should
reduce
symptoms and decrease the need
for bronchodilators (inhaled,
short-acting beta-agonists). Spacer
devices are recommended for children using
metered-dose
inhalers (MDI). The patient
should
rinse his or her mouth
after using Monitoring the patient's inhalation
technique is
an essential part of the asthma visit. Response
to therapy should be carefully monitored.
If
clear benefit is not observed,
alternative therapies should
be attempted, or other diagnoses,
such as chronic sinusitis,
should
be considered. Once
control of asthma symptoms is established and
sustained,
a careful step-down in therapy
should be attempted. Allergic
and irritant triggers play a prominent
role for
most children with daily asthma, as
well as for those with
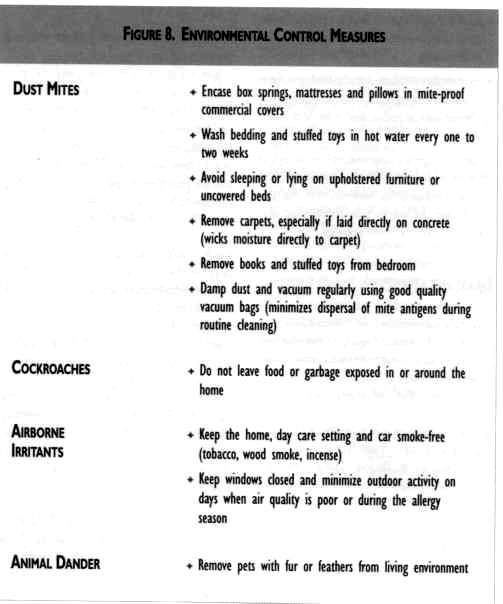
seasonal asthma. Environmental
controls are important in the
long-term management of
asthma, as they can decrease
the need for medications. Prompt
reassessment of asthma management is needed
after
any
asthma-related
hospitalization. or ernergency department.
after-hours, or urgent
carevisit. Spacer devices are recommended for children using
metered-dose
inhalers (MDI). It
is possible for most children with asthma to
lead normal
active lives and
avoid
emergency room visits
and hospitalizations. An
important goal is to eliminate, or reduce to a
minimum,
the need for
daily,
short-acting
beta-agonists (except pre-exercise). Through
an increased reliance on anti-inflammatorv
medications
and an emphasis on
environmental
control and
patient self-management, it
is possible for most children with
asthma to lead normal, active
lives and avoid emergency
room visits and hospitalizations. The
goals of asthma therapy are to: Prevent
symptoms that may interfere with daily
living
(e.g. school attendance, normal physical
activity, uninterrupted sleep)
Prevent
exacerbations of asthma, minimizing the
need for
emergency department visits or
hospitalizations Reduce
the risk of death Restore
and maintain normal, or best possible,
lung function Restore
normal peak flow variability; that is,
keep morning
peak flow within 80-100% of
personal
best Eliminate, or reduce to a minimum, the
need for
daily, short-acting beta-agonists
(except pre-exercise)
Provide optimal pharmacotherapy and prevent
adverse effects
from drug? Empower patients/parents to manage the disease
properly
and effectively Meet
patients' and families' expectations of their
asthma
care Symptoms of asthma can vary widely among
individual patients
and may mimic those present
in
other disease states. An
accurate diagnosis is essential
to effective management. To establish a
diagnosis of asthma, the
clinician should determine that: episodic
symptoms of airway obstruction are present airflow
obstruction is at least partially
reversible alternate diagnoses are excluded
Consider
a diagnosis of asthma if any of the
indicators
in Figure I are present. These
indicators are not diagnostic
by themselves, but the
presence of multiple, key indicators increases
the probability of an asthma
diagnosis. Spirometry or
peak expiratory flow before and
after bronchodilator use helps
to establish a diagnosis
of asthma in Questionable cases.
FIGURE I, KEY INDICATORS FOR CONSIDERING A
DIAGNOSIS OF
ASTHMA
Wheeling (Note that a
normal chest examination
and the absence of wheezing do
not exclude asthma.)
History
of any of the following: Cough,
particularly
when worse
at night Recurrent
wheeze Recurrent difficulty
in breathing Recurrent
chest tightness Revenible
airflow limitation and diumal variation
as measured
by a peak flow meter.
For
example: the peak
expiratory flow (PEF) measurement
in the morning (before taking an
inhaled short-acting
beta-agonist) varies 20% or more
when compared to the PEP measurement in
the early afternoon (after
taking an inhaled short-acting
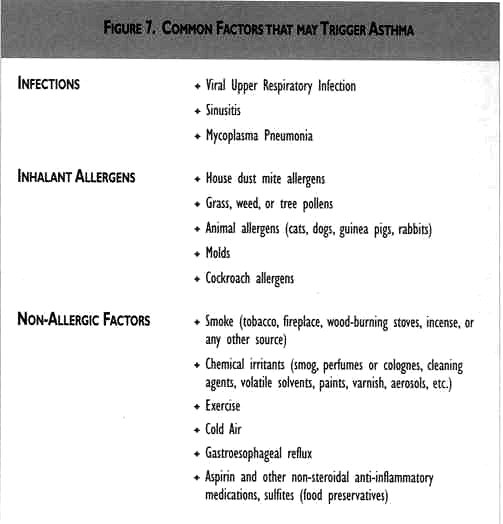
beta-agonist). Symptoms
occur or worsen in the presence of any of
the
following: Exercise
Viral infections
Animals with fur or feathers
House-dust mites (in
mattresses, pillows, upholstered
furniture, carpets)
Mold
Smoke (tobacco, wood)
Pollen
Changes in weather
Strong emotional expression
(laughing or crying hani)
Airborne
chemicals or dust
Menses
Symptoms
occur or worsen
at night, awakening
the patient Eczema.
hay fever, or a family history
of asthma or atopic
diseases are often associated with asthma,
but they are not key
indicators. A
normal chest exammation and the absence of
wheezing
do not exclude asthma. It
is recommended that peak flow be measured at
all asthma
visits,
both to
track progression of
the disease and to ensure
that the patient
is
using thepeak flow meter
correctly. ASSESSMENT and CLASSIFICATION of DISEASE
SEVERITY
The
recommended therapy for
asthma varies with the severity
of the disease. Severity should be
assessed between flares. It
can be estimated by objective
criteria and/or by symptoms. FEV1,
the forced volume of
air expired from
full inspiration in one second, measured with
spirometry, is considered the
single best measure of
airflow obstruction because it is sensitive in
both large and small airways.
An alternate measure, peak
expiratory flow rate (PEF or peak
flow), is only sensitive to
airflow in the large airways.
However, it correlates quite well with the
FEV1
and can be assessed with a simple, readily
accessible peak flow meter. A practical measure
for both home and clinician's
office, peak flow rate
is useful for assessing trends over time;
identifying asthma flares in
their early stages; monitoring
the effects of therapy; and identifying
triggers. Peak
flow tends to be lowest in the early morning
and
highest at midday. Daily peak flow variability
correlates well with airway
hyperactivity and is an important
characteristic of asthma that cannot be
assessed by a single
determination of FEV1.
Aggressive asthma therapy with oral and/or
inhaled corticosteroids may be
needed to establish the
personal best PEF. See the Tool Kit for
Practical Advice for
Treating Asthma in Children. Tables
with predicted peak flow values are
available (see
Tool Kit). However, it is best to rely
on the patient's own "personal
best" peak flow, particularly
if it is higher than the predicted value.
Appropriate management and a
high index of suspicion
that the child is unstable may reveal a
best peak flow value as high
as 150% of the predicted
value. On the other hand, when the best
peak flow is less than
predicted, and there is a suspicion
that best lung function has not been
achieved, it may be prudent to
judge severity based on
the predicted value. It
is recommended that peak flow be measured at
all asthma
visits, both to track progression of the
disease and to ensure that the
patient is using the peak
flow meter correctly. Have patients bring
their own peak flow meters to
visits since different
brands of peak flow meters give different readings.
|