
 Kaiser Diagnostic and
Treatment
Documents
Kaiser Diagnostic and
Treatment
Documents
 Kaiser Permanente Clinical
Practice Guidelines for Community Acquired
Pneumonia
Kaiser Permanente Clinical
Practice Guidelines for Community Acquired
Pneumonia
Clinical Guidelines for Community Acquired Pneumonia endorsed by https://kaiserpapers.com/downey/cajud/pnue/ Hospital Based Specialists Peer Group Chiefs of Infectious Disease Chiefs of Medicine Chiefs of Pulmonology Issued December 1998
KAISER PERMANENTE
The Permanente Medical Group (TPMG) Clinical Practice Guidelines have been developed to assist clinicians by providing an analytical framework for the evaluation and treatment of selected common problems encountered in patients. These guidelines are not intended to establish a protocol for all patients with a particular condition. While the guidelines provide one approach to evaluating a problem, clinical conditions may vary significantly from individual to individual. Therefore, the clinician must exercise independent judgment and make decisions based upon the situation presented.
While great care has been taken to assure the accuracy of the information presented, the reader is advised that TPMG cannot be responsible for continued currency of the information, for any errors or omissions in this guideline, or for any consequences arising from its use.
COMMUNITY ACQUIRED PNEUMONIA CLINICAL PRACTICE GUIDELINES TEAM https://kaiserpapers.com/downey/cajud/pnue/ CLINICAL LEADER Mark Clark, MD,HBS,Vallejo CPG TEAM David Goya, MD, Pulmonology, Santa Clara Chinh Le, MD, Infectious Disease, Santa Rosa Nada Ferns, NP, Medicine, Hayward PROJECT MANAGEMENT Jay Krishnaswamy, MBA, TPMG Department of Quality and Utilization Linda Rogers, MPA, TPMG Department of Quality and Utilization EDITING The Medical Editing Department, Kaiser Foundation Research Institute REVIEWERS Norman Absar, MD, HBS, Vallejo Henry Brodkin, MD, Medicine, Redwood City Melanio Castro, MD, HBS, Stockton Doug Chartier, MD, HBS, Oakland Deborah Chiarucci, MD, HBS, Redwood City Diane Craig, MD, HBS, Santa Clara Mike Driscoll, DO, HBS, Sacramento Louis Edelson, MD, HBS, Hayward Paul Feigenbaum, MD, Medicine, San Francisco Jerry Fessler, MD, HBS, Stockton John Fitzgibbon, MD, HBS, Sacramento Lauren Freeman, MD, HBS, South Sacramento William Geisser, MD, HBS, Fresno Dale Grahn, MD, HBS, Park Shadelands Brian Hoberman, MD, HBS, San Francisco Jianfei Hu, MD, HBS, Walnut Creek Aye Koko, MD, HBS, Fresno Pansy Kwong, MD, Medicine, Oakland Lewis Lehman, MD, HBS, San Francisco Janice Manjuck, MD, HBS, San Francisco Greg Matsubara, MD, HBS, Fresno Susanne Mierendorf, MD, HBS, Santa Clara Joseph Murphy, MD, Medicine, South San Francisco Bein Nguyen, MD, HBS, Santa Teresa Keith Palmer, MD, HBS, San Francisco Rita Patel, MD, HBS, Hayward Andrew Pollock, MD, HBS, Sacramento Robert Reisenfeld, MD, HBS, Walnut Creek Thomas Tang, MD, HBS, Redwood City Tien Trinh, MD, HBS, Santa Teresa Than Tran, MD, HBS, Stockton Abdul Wali, MD, HBS, Walnut Creek Albert Wilbum, MD, HBS, Fresno Thein Win, MD, HBS, Walnut Creek Joseph Wong, MD, HBS, Stockton Terry Woodard, MD, HBS, Santa Rosa DESIGN & PRODUCTION
Gail Holan. Curvey
To obtain more information about KPNC Clinical Practice Guidelines, printed copies, or permission to reproduce any portion, please contact TPMG Department of Quality & Utilization at 510-987-2950 or tie-line 8-427-2950, or send an e-mail message to clinical.guidelines@ncal.kaiperm.org. Within the KPNC Lotus Notes network mail to clinical guidelines or kpnc-cpg. KPNC Clinical Practice Guidelines can be viewed on- line on the Kaiser Permanente Northern California intranet website at http://clinical-library.ca.kp.org.
Ratified by the Operations Management Group and the Quality Oversight Committee Copyright 1998 The Permanente Medical Group, Inc.
CLINICAL PRACTICE GUIDELINES FOR COMMUNITY ACQUIRED PNEUMONIA
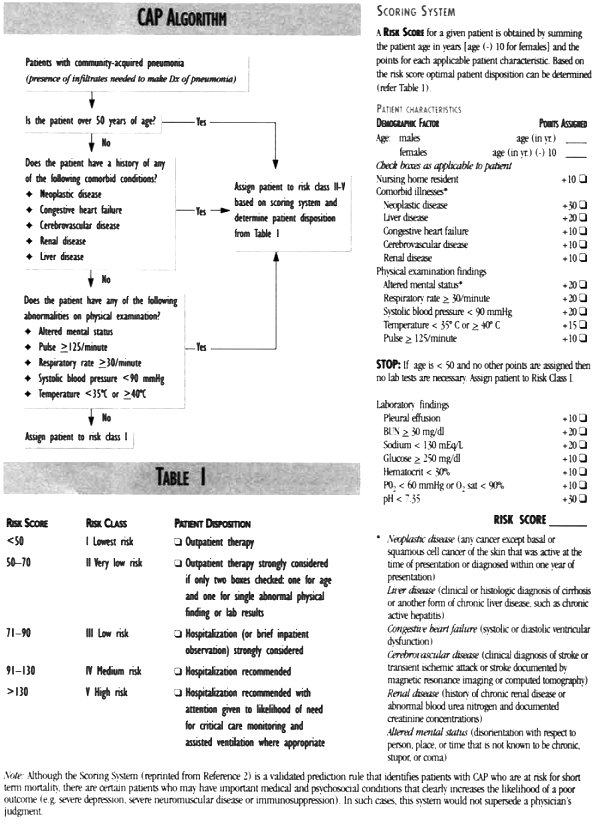
Hospital based physicians and clinician-managers can be guided by admission criteria, evaluaton and treatment recommendations, discharge criteria, expected measurable quality outcomes (such as cure rate or mortality rate), and utilization outcomes (such as length of stay) 1 Understanding of these issues as they pertain to community acquired pneumonia (CAP) has progressed, in recent years, to the point that certain evidence-based recommendations and predictions can be confidently made.
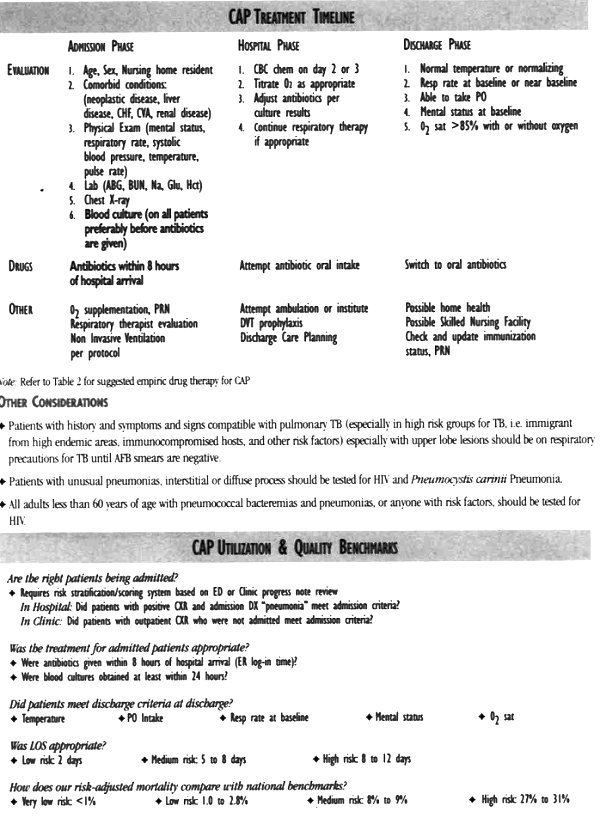
We can now predict, based upon the initial history, physical findings, and laboratory evaluation, which patients are likely to benefit from hospitalization for community acquired pneumonia.2 This has led to a set of well validated admission criteria for CAP, and allows us to forecast expected mortality and length of stay based on the risk of mortality estimated at the time of admission. Such a risk-adjusted approach takes into account the presence of other comorbid conditions, which may also be active 3, 4, 5 Thus, these recommendations and predictions are applicable to the complicated patients with CAP in our hospitals today. Certain interventions, such as early IV antibiotic administration and obtaining of blood cultures have been shown to have a beneficial effect on outcomes6Recommendations based on such evidence, and on strong consensus among treating physicians form the basis of this guideline. Where scientific evidence or strong consensus does not exist, no recommendations have been made. Where evidence does exist (e.g., in the admission decision or "door to needle time") such recommendations are given special prominence and may become the focus of quality monitoring.7
BACK to Kaiser Diagnostic and Treatment Documents Index